
Study: Growing Drug Rebates Hurt Both Consumers and Healthcare System
Promise of large rebates hikes co-pays, causes delays and access restrictions, and discourages use of more cost-effective drugs
BOSTON – Ever-larger rebates are distorting the market for branded drugs and producing outcomes that often benefit neither consumers nor the healthcare system, according to a new study published by Pioneer Institute.
Moreover, media coverage of drug pricing tends to ignore the growing role of rebates and therefore presents a somewhat erroneous picture of the key issues for patients such as growing out-of-pocket costs caused by rebates.
Manufacturers of new drugs routinely approach pharmaceutical benefit managers (PBMs), who represent one or more health plans. They promise that if the PBM can achieve, for example, a 30 percent market share for the new drug, the manufacturer will pay the PBM a sum equal to 40 percent of the drug’s list price.
“For a somewhat expensive drug, it wouldn’t be unusual for the rebate amount to be $90 million for the first quarter and $360 million for a year,” said Dr. William S. Smith, author of “Five Reasons Why Drug Rebates Are Harmful to Patients and to the Healthcare System.”
Rebates can cause PBMs to place restrictions on competing drugs. They include step therapy, which requires patients to “step” through cheaper drugs before getting to the one their doctor prescribed; prior authorizations, which require extensive paperwork for approvals to be granted; “fail first,” under which patients must fail on cheaper drugs before getting a more expensive one; and tiering, which sets much higher out-of-pocket costs for certain types of drugs.
The oncology community has been particularly outspoken in its criticism of these practices, which can cause treatment delays that result in poorer outcomes or even death.
The size of drug manufacturer rebates has been growing. One recent study found that the average rebate increased from 32 percent of list price in 2012 to 48 percent in 2017.
There is considerable evidence that rebates encourage manufacturers to assign higher list prices to new drugs. One study pegged annual list price inflation at 12 percent, while net inflation was just 3 percent.
List price inflation hurts patients, because co-pays are based on list prices. Imagine that the co-pay is 10 percent of list price for a drug that lists for $1,000, and for which the PBM receives the average 48 percent rebate. The consumer would have a $100 co-pay rather than the $52 that equals 10 percent of the drug’s actual $520 price after the rebate.
Increasing rebate amounts have also produced something called spread pricing. Under this practice, a PBM has a contract to be paid $100 whenever a particular drug is dispersed to a patient. The PBM then signs a contract to reimburse a retail pharmacy $75 and keeps the $25 “spread.” Some states have prohibited spread pricing, but it remains permissible under federal law.
Rebates only apply to branded drugs, since the profit margins on generics are too thin to allow for them. But rebates are increasingly knocking far cheaper generics out of the preferred tier of drugs with the lowest co-pays.
They are also limiting the use of biosimilars which, unlike generics, are not identical to the branded drugs, but are pharmaceutically “equivalent” and could materially reduce overall drug prices.
With the growth of expensive specialty drugs that treat rare conditions, biosimilars make up only 2 percent of U.S. prescriptions, but they account for 37 percent of drug spending.
Because they are more expensive to manufacture, discounts on biosimilars are far less than the 95 percent for some generic drugs. One study estimated biosimilar discounts at 10 percent to 37 percent. This means that once rebates are included, PBMs may prefer the originator drug to a biosimilar, even though that increases overall healthcare system costs.
Dr. Smith writes that it’s difficult to draw firm conclusions about the impact of rebates because both rebate levels and the negotiations that produce them are completely opaque. While he doesn’t recommend making rebate levels transparent because it may limit the discounts offered, he does recommend more public education regarding formulary design, out-of-pocket costs and how rebates affect overall drug prices.
The need for better public education led Dr. Smith to review a sample of 100 media stories that came up from a Google search on drug prices. The stories were selected at random, but an effort was made to select both national and regional articles with some emphasis on New England media outlets.
The review found that the media is generally performing poorly when it comes to explaining the decisive role rebates play in drug pricing. Overall, 64 percent of the stories sampled didn’t mention rebates.
Some outlets performed better. The majority of Wall Street Journal articles on drug prices discussed the rebate issue, as did 7 of 13 Boston Globe articles on the topic. Others, including The Economist and The New York Times didn’t mention rebates in any of the stories sampled.
About the Author
Dr. William S. Smith is Visiting Fellow in Life Sciences at Pioneer Institute. He writes about public policy issues impacting the life sciences industry with particular emphasis upon pharmaceuticals. Dr. Smith has 25 years of experience in government and in corporate roles. He spent ten years at Pfizer as Vice President of Public Affairs and Policy. He later served as a consultant to major pharmaceutical, biotechnology and medical device companies, and was President of a small medical device company for three years. His career has also included senior staff positions for the Republican House leadership on Capitol Hill, the White House, and in the Governor’s office in Massachusetts. He is affiliated as Research Fellow and Managing Director with the Center for the Study of Statesmanship at The Catholic University of America (CUA). He earned his PhD at CUA and a bachelor’s degree from Georgetown University.
About Pioneer
Mission: Pioneer Institute develops and communicates dynamic ideas that advance prosperity and a vibrant civic life in Massachusetts and beyond.
Vision: Success for Pioneer is when the citizens of our state and nation prosper and our society thrives because we enjoy world-class options in education, healthcare, transportation and economic opportunity, and when our government is limited, accountable and transparent.
Values: Pioneer believes that America is at its best when our citizenry is well-educated, committed to liberty, personal responsibility, and free enterprise, and both willing and able to test their beliefs based on facts and the free exchange of ideas.
Get Updates On Our Life Sciences Work!
Related Content
 https://pioneerinstitute.org/wp-content/uploads/Patents-arent-evil.png
512
1024
William Smith
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
William Smith2023-05-15 13:12:342023-05-31 11:45:08Opinion: Drug patents aren’t a ‘necessary evil.’ They save lives.
https://pioneerinstitute.org/wp-content/uploads/Patents-arent-evil.png
512
1024
William Smith
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
William Smith2023-05-15 13:12:342023-05-31 11:45:08Opinion: Drug patents aren’t a ‘necessary evil.’ They save lives. https://pioneerinstitute.org/wp-content/uploads/Copy-of-work-force.png
512
1024
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2023-05-15 09:00:202023-05-15 15:38:49Study: High List Prices and Deep Discounts for Prescription Drugs Hurt Poor and Sick Patients
https://pioneerinstitute.org/wp-content/uploads/Copy-of-work-force.png
512
1024
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2023-05-15 09:00:202023-05-15 15:38:49Study: High List Prices and Deep Discounts for Prescription Drugs Hurt Poor and Sick Patients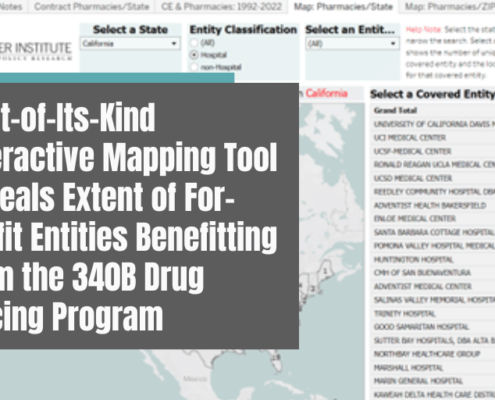 https://pioneerinstitute.org/wp-content/uploads/Pioneer-Institute-Statement-on-Question-1-1.png
512
1000
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2023-01-11 07:43:522023-01-11 07:44:28First-of-Its-Kind Interactive Mapping Tool Reveals Extent of For-Profit Entities Benefitting from the 340B Drug Pricing Program
https://pioneerinstitute.org/wp-content/uploads/Pioneer-Institute-Statement-on-Question-1-1.png
512
1000
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2023-01-11 07:43:522023-01-11 07:44:28First-of-Its-Kind Interactive Mapping Tool Reveals Extent of For-Profit Entities Benefitting from the 340B Drug Pricing Program https://pioneerinstitute.org/wp-content/uploads/340-web-post.png
900
1600
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2022-03-22 05:41:312022-03-25 14:38:00Massachusetts Hospitals Pull Back on Charity Care as Revenue from Federal 340B Drug Discount Program Explodes
https://pioneerinstitute.org/wp-content/uploads/340-web-post.png
900
1600
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2022-03-22 05:41:312022-03-25 14:38:00Massachusetts Hospitals Pull Back on Charity Care as Revenue from Federal 340B Drug Discount Program Explodes https://pioneerinstitute.org/wp-content/uploads/Untitled-design-2021-12-06T120924.383.png
512
1024
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2021-12-06 11:44:202021-12-06 12:10:01The Promise and Challenges of Rare Cancer Treatments
https://pioneerinstitute.org/wp-content/uploads/Untitled-design-2021-12-06T120924.383.png
512
1024
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2021-12-06 11:44:202021-12-06 12:10:01The Promise and Challenges of Rare Cancer Treatments https://pioneerinstitute.org/wp-content/uploads/NEW-REPORT.png
512
1024
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2021-11-09 05:39:002021-11-09 05:41:06Study: Decline in Cardiovascular Health Screenings During COVID-19 Pandemic Poses New Public Health Threat
https://pioneerinstitute.org/wp-content/uploads/NEW-REPORT.png
512
1024
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2021-11-09 05:39:002021-11-09 05:41:06Study: Decline in Cardiovascular Health Screenings During COVID-19 Pandemic Poses New Public Health Threat https://pioneerinstitute.org/wp-content/uploads/The-QALY-and-Cancer-Treatments_-An-Ill-Advised-Match.png
512
1024
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2021-04-06 04:45:242021-07-19 10:41:05New Analysis: ICER Framework Ignores Patient Preferences, Innovation & Societal Benefits in Evaluating Cost-Effectiveness of New Cancer Treatments
https://pioneerinstitute.org/wp-content/uploads/The-QALY-and-Cancer-Treatments_-An-Ill-Advised-Match.png
512
1024
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2021-04-06 04:45:242021-07-19 10:41:05New Analysis: ICER Framework Ignores Patient Preferences, Innovation & Societal Benefits in Evaluating Cost-Effectiveness of New Cancer Treatments https://pioneerinstitute.org/wp-content/uploads/Five-Reasons-Why-Drug-Rebates-Are-Harmful-to-Patients-and-to-the-Healthcare-System-4.png
512
1024
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2020-10-20 11:20:432020-12-10 16:24:25Study: Growth of Antibiotic-Resistant Infections Could Have Massive Human, Financial Costs
https://pioneerinstitute.org/wp-content/uploads/Five-Reasons-Why-Drug-Rebates-Are-Harmful-to-Patients-and-to-the-Healthcare-System-4.png
512
1024
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2020-10-20 11:20:432020-12-10 16:24:25Study: Growth of Antibiotic-Resistant Infections Could Have Massive Human, Financial Costs https://pioneerinstitute.org/wp-content/uploads/Five-Reasons-Why-Drug-Rebates-Are-Harmful-to-Patients-and-to-the-Healthcare-System.png
512
1024
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2020-09-01 06:40:182020-12-11 12:09:06Study: Growing Drug Rebates Hurt Both Consumers and Healthcare System
https://pioneerinstitute.org/wp-content/uploads/Five-Reasons-Why-Drug-Rebates-Are-Harmful-to-Patients-and-to-the-Healthcare-System.png
512
1024
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2020-09-01 06:40:182020-12-11 12:09:06Study: Growing Drug Rebates Hurt Both Consumers and Healthcare System https://pioneerinstitute.org/wp-content/uploads/Fresh-Aqua-Summit-1.png
512
1024
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2020-05-21 05:48:362021-11-23 10:32:03Study Finds Pandemic Likely to Negatively Impact Biopharmaceutical Sector
https://pioneerinstitute.org/wp-content/uploads/Fresh-Aqua-Summit-1.png
512
1024
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2020-05-21 05:48:362021-11-23 10:32:03Study Finds Pandemic Likely to Negatively Impact Biopharmaceutical Sector
