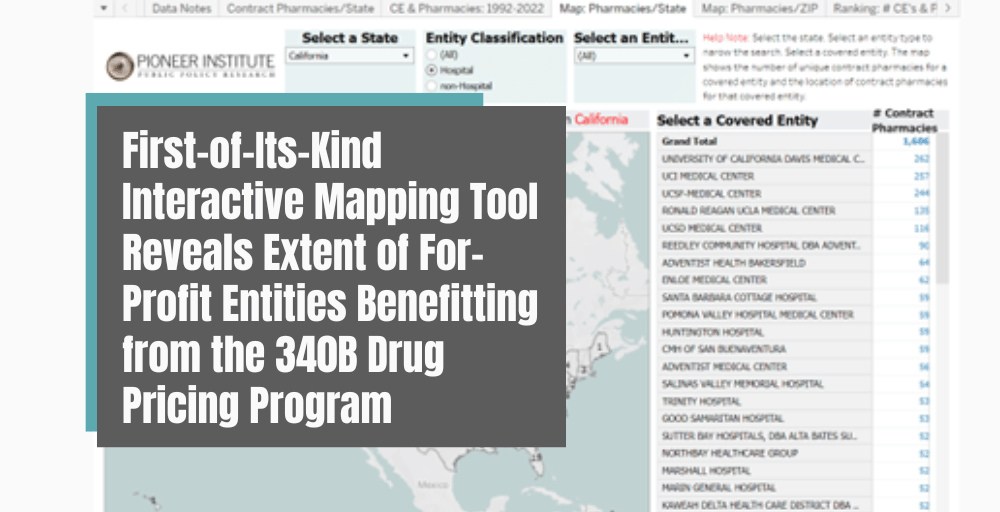
First-of-Its-Kind Interactive Mapping Tool Reveals Extent of For-Profit Entities Benefitting from the 340B Drug Pricing Program
Pioneer Institute Database Spotlights How 340B Covered Entities Utilize Thousands of Out-of-State Contract Pharmacies to Turn Profits in Program Intended to Serve Vulnerable Patients
JANUARY 11, 2023 (BOSTON, MA) – Today, Pioneer Institute released a first-of-its-kind, 50-state mapping tool and database highlighting the troubling way in which hospitals and covered entities leverage unlimited pharmacy contracts under the 340B Drug Pricing Program. Authored by Dr. Bill Smith and Dr. Robert Popovian, the easy-to-use tool and database enables policymakers, legislators, researchers, and practitioners to see the number and location of contract pharmacies for 340B covered entities in all 50 states. Pioneer Institute data visualizations illustrate the growth in the web of for-profit entities now benefitting from the 340B program, a program intended to benefit the most vulnerable patient populations.
The mapping tool features interactive data visualizations that shed light on how 340B entities have taken advantage of the contract pharmacy arrangement, including:
- Zip code level mapping of the number of contract pharmacies in each state for every 340B covered entity, spotlighting the number of out-of-state pharmacies in high-income areas.
- State level mapping of contract pharmacy relationships for every 340B covered entity.
- Growth of contract pharmacy relationships with 340B covered entities since 1992, in all 50 states, including unique contract pharmacies and active contracts with those pharmacies.
“While the 340B program was created with good intentions, evidence continues to show that the program has enormous potential for abuse by for-profit pharmacy chains and pharmacy benefit managers,” said Dr. Bill Smith, Senior Fellow and Director of the Life Sciences Initiative at Pioneer Institute and primary author of the Pioneer tool. “This new tool lays bare how convoluted the 340B program is in design and how for-profit entities are now some of the principal beneficiaries of the program.”
The 340B Drug Pricing Program was established as a federal safety-net program to offer discounts on healthcare treatments to low-income and uninsured populations. In 1996, the Health Resources and Services Administration (HRSA) issued guidance allowing 340B hospitals and other covered entities to dispense 340B drugs through an in-house pharmacy or a single external pharmacy. However, in 2010, HRSA updated its guidance to allow covered entities to contract with an unlimited number of pharmacies to purchase and dispense 340B drugs. As a result, the number of 340B contract pharmacy arrangements has exploded by 4,000% since 2010. As many as 73% of 340B contract pharmacies are large for-profit chains and pharmacy benefit managers.
“The mapping tool clearly demonstrates that powerful hospitals have established tens of thousands of contracts with for-profit entities who are securing enormous profits from the 340B program,” said Dr. Robert Popovian, Senior Visiting Health Policy Fellow at Pioneer Institute and co-author of the Pioneer tool. “There must be increased oversight of 340B covered entities’ use of contract pharmacy relationships to return the program to its original intent of supporting the most vulnerable patients.”
The scope and number of contract pharmacies create an enormous potential for abuse as pharmacies can drive profits by charging multiple discounts, such as purchasing drugs at 340B discounts and billing drug manufacturers for Medicaid rebates on the same drug, known as duplicate discounts. While duplicate discounts violate federal law, and government watchdogs have requested that pharmacies install tools to prevent them, pharmacy chains have not heeded these government requests.
Federal and state legislators and regulators can utilize this new tool to investigate, down to the zip code level, and better grasp how 340B contract pharmacies are taking advantage of the program. Recent research concluded that 340B contract pharmacy growth was concentrated in high-income neighborhoods, compared to low-income communities where the number of contract pharmacies declined.
- Cambridge Public Health Commission, a Massachusetts-based healthcare system, has 349 contract pharmacies in the state. However, it also has 11 contract pharmacies in California, 11 in Florida, and many more across the country.
- In Virginia, Bon Secours Richmond Community Hospital, recently the subject of an investigation into their misuse of 340B drug discounts, has a contract pharmacy in Florida and one in Arizona, in addition to contract pharmacies in neighboring states.
To view the Pioneer Institute 340B interactive mapping tool, visit https://pioneerinstitute.org/340babuse/.
###
About the Authors
Dr. William S. Smith is Senior Fellow and Director of the Life Sciences Initiative at Pioneer Institute. He has 25 years of experience in government and in corporate roles, including as vice president of public affairs and policy at Pfizer, and as a consultant to major pharmaceutical, biotechnology and medical device companies. He held senior staff positions for the Republican House leadership on Capitol Hill, the White House, and in the Massachusetts Governor’s office. He earned his PhD with distinction at The Catholic University of America (CUA).
Dr. Robert Popovian is Senior Visiting Health Policy Fellow at Pioneer Institute. Dr. Popovian is the Founder of the strategic consulting firm Conquest Advisors. He previously served as Vice President, U.S. Government Relations at Pfizer. Dr. Popovian was appointed as the Chief Science Policy Officer for Global Healthy Living Foundation. He also serves on the Board of Councilors of the University of Southern California School of Pharmacy, Senior Health Policy Fellow at Progressive Policy Institute, and Board of Advisors for Equideum Health. Robert completed his Doctorate in Pharmacy and Master of Science in Pharmaceutical Economics and Policy degrees at the University of Southern California with honors.
Gauri Binoy is a research assistant at Pioneer Institute. She graduated from Cornell University with a BA in Biological Sciences and Developmental Sociology in May 2021.
About Pioneer Institute
Pioneer’s mission is to develop and communicate dynamic ideas that advance prosperity and a vibrant civic life in Massachusetts and beyond. Pioneer’s vision of success is a state and nation where our people can prosper and our society thrive because we enjoy world-class options in education, healthcare, transportation and economic opportunity, and where our government is limited, accountable and transparent. Pioneer values an America where our citizenry is well-educated and willing to test our beliefs based on facts and the free exchange of ideas, and committed to liberty, personal responsibility, and free enterprise.
Get Updates On Our Life Sciences Work!
Related Content
 https://pioneerinstitute.org/wp-content/uploads/credit-card-5.png
512
1024
William Smith
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
William Smith2020-05-21 15:11:042020-06-29 13:05:55The Negative Impact of COVID-19 Upon the Biopharmaceutical Sector
https://pioneerinstitute.org/wp-content/uploads/credit-card-5.png
512
1024
William Smith
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
William Smith2020-05-21 15:11:042020-06-29 13:05:55The Negative Impact of COVID-19 Upon the Biopharmaceutical Sector https://pioneerinstitute.org/wp-content/uploads/Fresh-Aqua-Summit-1.png
512
1024
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2020-05-21 05:48:362021-11-23 10:32:03Study Finds Pandemic Likely to Negatively Impact Biopharmaceutical Sector
https://pioneerinstitute.org/wp-content/uploads/Fresh-Aqua-Summit-1.png
512
1024
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2020-05-21 05:48:362021-11-23 10:32:03Study Finds Pandemic Likely to Negatively Impact Biopharmaceutical Sector https://pioneerinstitute.org/wp-content/uploads/Green-Grunge-Basketball-Quote-UAAP_NCAA-Twitter-Post-1.png
512
1024
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2020-04-02 06:00:242020-12-11 13:28:28New Report: Quality Adjusted Life Years (QALY) Methodology Discriminates Against Older Americans, Threatens to Deny Seniors Access to Life-Saving Care
https://pioneerinstitute.org/wp-content/uploads/Green-Grunge-Basketball-Quote-UAAP_NCAA-Twitter-Post-1.png
512
1024
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2020-04-02 06:00:242020-12-11 13:28:28New Report: Quality Adjusted Life Years (QALY) Methodology Discriminates Against Older Americans, Threatens to Deny Seniors Access to Life-Saving Care https://pioneerinstitute.org/wp-content/uploads/credit-card-17.png
512
1024
William Smith
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
William Smith2020-03-31 16:22:382021-11-23 10:48:57Quality Adjusted Life Years (QALY): The Threat to Older Americans
https://pioneerinstitute.org/wp-content/uploads/credit-card-17.png
512
1024
William Smith
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
William Smith2020-03-31 16:22:382021-11-23 10:48:57Quality Adjusted Life Years (QALY): The Threat to Older Americans https://pioneerinstitute.org/wp-content/uploads/ElderNursingHome.jpg
420
630
Jim McKenna
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Jim McKenna2020-02-10 16:36:592021-11-23 10:33:49The Legality of QALY under the ADA
https://pioneerinstitute.org/wp-content/uploads/ElderNursingHome.jpg
420
630
Jim McKenna
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Jim McKenna2020-02-10 16:36:592021-11-23 10:33:49The Legality of QALY under the ADA https://pioneerinstitute.org/wp-content/uploads/1140-man-wheelchair-disability-aarp.imgcache.rev5804edef486e77e680d3985a3ddb67dd.jpg
655
1140
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2020-02-10 07:00:262021-01-28 15:07:32New Report & Legal Analysis Suggests ICER’s Quality Adjusted Life Years Methodology Violates the Americans with Disabilities Act
https://pioneerinstitute.org/wp-content/uploads/1140-man-wheelchair-disability-aarp.imgcache.rev5804edef486e77e680d3985a3ddb67dd.jpg
655
1140
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2020-02-10 07:00:262021-01-28 15:07:32New Report & Legal Analysis Suggests ICER’s Quality Adjusted Life Years Methodology Violates the Americans with Disabilities Act https://pioneerinstitute.org/wp-content/uploads/icerwatch.png
400
800
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2019-06-26 00:00:252019-07-24 15:03:20Report: Rare Disease Patients Hurt by “One-Size-Fits-All” ICER Framework
https://pioneerinstitute.org/wp-content/uploads/icerwatch.png
400
800
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2019-06-26 00:00:252019-07-24 15:03:20Report: Rare Disease Patients Hurt by “One-Size-Fits-All” ICER Framework https://pioneerinstitute.org/wp-content/uploads/questionmark-of-pills.jpg
599
900
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2019-06-24 00:01:552019-07-31 15:57:22New Report Addresses Distinct Challenges in Utilizing ICER to Assess Value of Rare Disease Treatments
https://pioneerinstitute.org/wp-content/uploads/questionmark-of-pills.jpg
599
900
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2019-06-24 00:01:552019-07-31 15:57:22New Report Addresses Distinct Challenges in Utilizing ICER to Assess Value of Rare Disease Treatments https://pioneerinstitute.org/wp-content/uploads/Biotechnology.jpg
380
542
William Smith
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
William Smith2019-06-21 10:31:012020-06-29 13:34:53Looming Challenges for ICER in Assessing the Value of Rare Disease Therapies
https://pioneerinstitute.org/wp-content/uploads/Biotechnology.jpg
380
542
William Smith
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
William Smith2019-06-21 10:31:012020-06-29 13:34:53Looming Challenges for ICER in Assessing the Value of Rare Disease Therapies https://pioneerinstitute.org/wp-content/uploads/doctor-crossed-arms-1.jpg
1732
1733
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2019-06-12 00:00:392021-12-29 12:18:31Putting a Price on Life: The Coming Fight Over Government Rationing of Medical Care
https://pioneerinstitute.org/wp-content/uploads/doctor-crossed-arms-1.jpg
1732
1733
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2019-06-12 00:00:392021-12-29 12:18:31Putting a Price on Life: The Coming Fight Over Government Rationing of Medical Care
