Study: Massachusetts Should Embrace Direct Healthcare Options
RevCycle Intelligence: Direct Primary Care Increases Patient-Centered Care Access
Approach to investing in primary care yields lower costs, greater efficiency and increased patient satisfaction
BOSTON – Especially in the COVID era, many are looking to alleviate the increased burden on the healthcare system. One solution is direct healthcare (DHC), which can provide more patient-centered care at affordable prices and is an effective model to increase access to care for the uninsured, underinsured and those on public programs like Medicaid, according to a new study published by Pioneer Institute.
“This approach to investing in primary care has been shown to reduce costs, emergency room visits, inpatient care and visits to specialists, all while increasing patients’ satisfaction with their care,” said Josh Archambault, co-author with Greg George of “Direct Health Care Agreements: A New Option for Patient-Centered Care That Costs Less and Reduces Provider Burnout.”
Under DHC, patients pay practices a set monthly fee that covers a prearranged universe of services. It is most common in primary care, but can be used for other types of care such as physical therapy, behavioral and mental health, and dentistry. There are currently 1,200 direct primary care (DPC) practices in the U.S., at least 16 of which are in Massachusetts.
For primary care, patients begin by choosing their provider, then purchase a complementary insurance plan. They can usually buy a much less expensive plan with a higher deductible because they have access to so many services through DPC.
DPC agreements commonly include:
- Unlimited office visits
- Home visits
- Same- or next-day appointment availability
- Longer visit durations
- Annual physicals
- Vaccinations
- Routine lab tests
- Stitches and splintering or casting of fractured or broken bones
- Help navigating the rest of the healthcare system
- 24/7 emergency triage support
Some agreements include access to generic prescription drugs at near wholesale prices. Many DPC physicians give patients their personal cell phone numbers.
In 2018, nearly 80 percent of DPC subscription fees were between $51 and $99 per month, and costs have been stable over time. About 60 percent of patients who belong to a DPC practice have an annual household income of $95,000 or less.
One DPC provider shared the story of an uninsured 30-year-old man who pays $648 a year for access to the direct primary care practice. Since joining the practice the patient has suffered from a serious sinus infection, recurrence of cellulitis with abscesses that required draining, had multiple musculoskeletal injuries due to a car crash, and needed an x-ray for a possible femur fracture. The only additional cost to the patient for treatment of all these ailments was a $60 x-ray and inexpensive antibiotics. All other care was provided for under the $648. If he had sought care at the emergency room for any of the ailments, his bill for one visit would have been two or three times that amount.
There are no deductibles, co-pays or third-party insurance claims. The transparency and lack of surprise bills address the issue of those who don’t see their doctors because of uncertainty over the cost.
DPC patients have an average of four, 35-minute visits a year with their physician. Under the typical fee-for-service model, patients have 1.66 visits annually and spend around 15 minutes per visit with their physician.
DHC also results in far less physician burnout. “Status quo” providers currently report spending around a third of their day on administrative tasks, by contrast direct care providers spend much more time with patients because there is no paperwork to fill out for insurers.
DHC could help a number of patient groups. Access to same- or next-day appointments could be particularly helpful to MassHealth members. Pre-pandemic, the average wait for a doctor’s appointment in Boston was 50 days, and many providers don’t accept Medicaid.
Older adults on Medicare who often have trouble finding transportation to medical appointments could benefit from the home visits usually included in DPC agreements and from the more personal management of chronic illnesses that comes with longer and more frequent appointments.
A study published in the American Journal of Primary Care found that a small subset of direct health care arrangements studied resulted in a $119.4 million decrease in preventable hospital use in these practices in New York, Florida, Virginia, Arizona and Nevada. Over 90 percent of the savings – $2,551 per patient – came from Medicare patients.
DHC also offers an innovative option for small businesses. Superior Packaging and Finishing in Braintree saved $370,000 in a year, or over $4,300 per enrolled employee, when the company switched to offering a DPC plan to its employees.
Archambault urges the Commonwealth to take four steps to embrace DHC:
- Division of Insurance guidance should be updated to match 35 other states by clarifying that any form of direct care should not be regulated like insurance. If there was clear support, the Legislature could codify this standard.
- The Group Insurance Commission should embrace direct health care arrangements for public employees and offer it as a lower-cost option.
- MassHealth should explore DHC arrangements, especially for some of the sickest patients on the program.
- The Legislature could consider requiring that insurance companies offer at least one product to consumers that wraps around DHC arrangements, especially DPC. This reform would introduce a new, less-expensive option for consumers, as the product would have a higher deductible than most plans currently offered in Massachusetts.
About the Authors
Josh Archambault is a Senior Fellow at Pioneer Institute. Prior to joining Pioneer, Josh was selected as a Health Policy Fellow at the Heritage Foundation in Washington, D.C. In the past, Josh served as a Legislative Director in the Massachusetts State Senate and as Senior Legislative Aide in the Governor’s Office of Legislative Affairs. His work has appeared or been cited in outlets such as USA Today, Wall Street Journal, The New York Times, Fox News, NPR, Boston Herald and The Boston Globe. He is the editor and coauthor of The Great Experiment: The States, The Feds, and Your Healthcare. Josh holds a Master’s in Public Policy from Harvard University’s Kennedy School and a BA in Political Studies and Economics from Gordon College.
Greg George is the health policy and state affairs advisor for the Mackinac Center for Public Policy. Prior to joining Mackinac, Greg served as a senior research fellow at the Foundation for Government Accountability. He has also been a policy advisor for the Michigan House of Representatives and legislative director for the Michigan Speaker Pro Tempore. He holds a Bachelor of Science in Finance from Hillsdale College and a Master of Business Administration from Western Michigan University.
Pioneer’s mission is to develop and communicate dynamic ideas that advance prosperity and a vibrant civic life in Massachusetts and beyond.
Pioneer’s vision of success is a state and nation where our people can prosper and our society thrive because we enjoy world-class options in education, healthcare, transportation and economic opportunity, and where our government is limited, accountable and transparent.
Pioneer values an America where our citizenry is well-educated and willing to test our beliefs based on facts and the free exchange of ideas, and committed to liberty, personal responsibility, and free enterprise.
Get Updates On Our Healthcare Research and Events!
Related Posts
 https://pioneerinstitute.org/wp-content/uploads/Obama-and-Deval-2.jpg
275
315
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-09-30 13:30:382012-12-04 17:28:39Obama Admin Rethinking Massachusetts Model? Part 2
https://pioneerinstitute.org/wp-content/uploads/Obama-and-Deval-2.jpg
275
315
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-09-30 13:30:382012-12-04 17:28:39Obama Admin Rethinking Massachusetts Model? Part 2 https://pioneerinstitute.org/wp-content/uploads/locked-door.jpg
744
1150
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-09-14 17:24:382012-12-04 17:28:40Patrick Admin’s Misdiagnosis on ACA Transparency
https://pioneerinstitute.org/wp-content/uploads/locked-door.jpg
744
1150
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-09-14 17:24:382012-12-04 17:28:40Patrick Admin’s Misdiagnosis on ACA Transparency https://pioneerinstitute.org/wp-content/uploads/hef-and-kids.jpg
201
251
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-09-09 11:58:102012-12-04 17:28:44Are ACOs designed to care for grandparents also good for their grandkids?
https://pioneerinstitute.org/wp-content/uploads/hef-and-kids.jpg
201
251
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-09-09 11:58:102012-12-04 17:28:44Are ACOs designed to care for grandparents also good for their grandkids?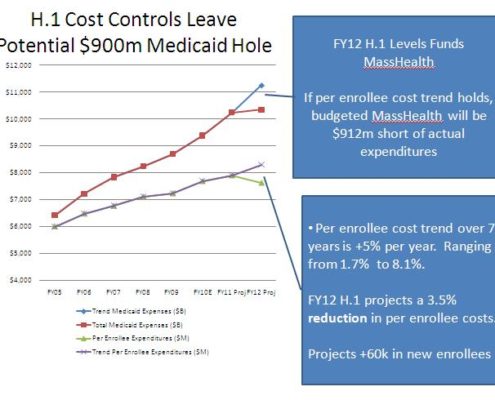 https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
0
0
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2011-09-08 16:06:392015-03-09 02:27:27A Fair and Cost Effective Tort System for Health Care
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
0
0
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-09-06 13:53:392012-12-04 17:28:49Does Your Doctor Know How Much That Costs?
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
0
0
Editorial Staff
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Editorial Staff2011-09-08 16:06:392015-03-09 02:27:27A Fair and Cost Effective Tort System for Health Care
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
0
0
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-09-06 13:53:392012-12-04 17:28:49Does Your Doctor Know How Much That Costs? https://pioneerinstitute.org/wp-content/uploads/Deval-and-Obama.jpg
297
450
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-09-01 15:01:482012-12-04 17:28:51Obama Admin Rethinking Massachusetts Model?
https://pioneerinstitute.org/wp-content/uploads/Deval-and-Obama.jpg
297
450
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-09-01 15:01:482012-12-04 17:28:51Obama Admin Rethinking Massachusetts Model? https://pioneerinstitute.org/wp-content/uploads/confused-bureaucrat.jpg
358
477
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-08-18 14:57:362012-12-04 17:28:51Governor, When is Excessiveness Excessive?
https://pioneerinstitute.org/wp-content/uploads/confused-bureaucrat.jpg
358
477
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-08-18 14:57:362012-12-04 17:28:51Governor, When is Excessiveness Excessive? https://pioneerinstitute.org/wp-content/uploads/wishful-thinking-t4763.jpg
750
531
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-08-16 14:33:542012-12-04 17:28:51Wishful Thinking On Romneycare & Obamacare for Employers
https://pioneerinstitute.org/wp-content/uploads/wishful-thinking-t4763.jpg
750
531
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-08-16 14:33:542012-12-04 17:28:51Wishful Thinking On Romneycare & Obamacare for Employers https://pioneerinstitute.org/wp-content/uploads/CMS-projections.bmp
610
1024
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-08-10 15:51:342012-12-04 17:28:53Massachusetts is 1st in the Nation on Health Care Cost!
https://pioneerinstitute.org/wp-content/uploads/CMS-projections.bmp
610
1024
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-08-10 15:51:342012-12-04 17:28:53Massachusetts is 1st in the Nation on Health Care Cost! https://pioneerinstitute.org/wp-content/uploads/plastic-surgery-error-cartoon.jpg
355
400
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-07-25 12:23:432016-09-06 08:17:12Do you feel safer in a hospital or on an airplane?
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
0
0
Taylor Armerding
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Taylor Armerding2011-07-12 17:16:232022-03-31 12:46:32Their Solution is Dilution
https://pioneerinstitute.org/wp-content/uploads/plastic-surgery-error-cartoon.jpg
355
400
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-07-25 12:23:432016-09-06 08:17:12Do you feel safer in a hospital or on an airplane?
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
0
0
Taylor Armerding
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Taylor Armerding2011-07-12 17:16:232022-03-31 12:46:32Their Solution is Dilution https://pioneerinstitute.org/wp-content/uploads/money-next-to-toilet.jpg
319
400
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-07-12 12:13:092012-12-04 17:28:55Feds Crapping Away Health $ and Increasing Deficit
https://pioneerinstitute.org/wp-content/uploads/money-next-to-toilet.jpg
319
400
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-07-12 12:13:092012-12-04 17:28:55Feds Crapping Away Health $ and Increasing Deficit https://pioneerinstitute.org/wp-content/uploads/VT-map-upside-down1.bmp
571
374
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-07-07 13:21:152013-04-09 10:06:16Vermont Single-Payer Plan Full of Holes
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
0
0
Jim Stergios
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Jim Stergios2011-07-05 14:41:192022-03-31 12:48:51Watch Me Pull A Rabbit Out of My Hat
https://pioneerinstitute.org/wp-content/uploads/Medicaid-projections.jpg
490
655
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-07-01 11:10:482012-12-04 17:28:59Beacon Hill’s Budget MassHealth Mirage
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
0
0
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-06-30 16:59:342012-12-04 17:29:04HCFA & GBIO’s Misdiagnosis
https://pioneerinstitute.org/wp-content/uploads/VT-map-upside-down1.bmp
571
374
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-07-07 13:21:152013-04-09 10:06:16Vermont Single-Payer Plan Full of Holes
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
0
0
Jim Stergios
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Jim Stergios2011-07-05 14:41:192022-03-31 12:48:51Watch Me Pull A Rabbit Out of My Hat
https://pioneerinstitute.org/wp-content/uploads/Medicaid-projections.jpg
490
655
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-07-01 11:10:482012-12-04 17:28:59Beacon Hill’s Budget MassHealth Mirage
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
0
0
Joshua Archambault
https://pioneerinstitute.org/wp-content/uploads/logo_440x96.png
Joshua Archambault2011-06-30 16:59:342012-12-04 17:29:04HCFA & GBIO’s Misdiagnosis