
An Evaluation of 340B in Massachusetts
Introduction
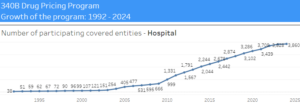
The 340B Drug Pricing Program is one of the country’s largest federal drug programs. Enacted in 1992, 340B requires drug manufacturers to sell drugs to eligible hospitals and clinics at a discounted rate. Aimed at reducing costs of prescription drugs for low-income and uninsured patients, the program has grown immensely over time.
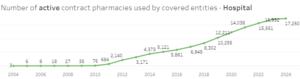
With an increase in the number of hospitals, clinics, and pharmacies using the program, and with the Affordable Care Act’s incentives for health care entities to participate, increased access to effective healthcare for vulnerable populations may seem like a reasonable expectation. Unfortunately, this has not been the case, as the 340B program has suffered from exploitation and a lack of transparency.
The 340B program has been abused across the country, but especially in Massachusetts. Although the Commonwealth is renowned for its medical research and hospitals, as well as being widely regarded as one of the largest biotech hubs in the world, the landscape of 340B in Massachusetts is bleaker than that of the rest of the country.
340B in Massachusetts
Despite the objective of making pharmaceuticals more accessible and affordable for low-income patients, 340B has had the opposite effect. Pioneer Institute has compiled an extensive database that illuminates the shortcomings of the program.
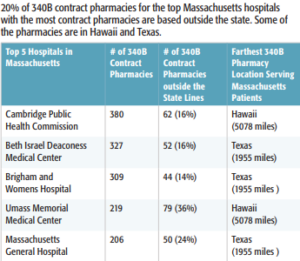
In Massachusetts, 61 percent of 340B pharmacies are located in high-income districts. Additionally, 21 percent of 340B pharmacies are located outside the state. Of the Massachusetts hospitals with the most 340B contract pharmacies, 20 percent of those contract pharmacies are located outside the state. Some low-income patients have to use pharmacies as far away as Texas and Hawaii.
Furthermore, charity care, which is allegedly the cornerstone of the 340B program, has actually decreased as the program has grown. In Massachusetts, the average charity care ratio for 340B hospitals was 0.95 percent in 2022. That is well below the national average of 2.28 percent. Massachusetts General Hospital, which has the highest operating expenses of any 340B-eligible hospital in the state, provided even less charity care in 2022 with a ratio of 0.6 percent.

Implications
Nationwide, drug purchases, at discounted prices, through 340B increased from $9 billion in 2014 to $38 billion in 2020. But as in Massachusetts, the program has expanded at the expense of charity care, as charity care ratios have fallen. Some claim the expansion of Medicaid has been a driving force behind the drop in charity care. But if there was a declining need for charity care, why did 340B expand so much?
Since Massachusetts hospitals are not required to report revenues for 340B drugs, there are no publicly available data on how much revenue each Massachusetts hospital brought in through 340B, which would be important to have. Among other things, the lack of transparency with 340B is leading to exploitation that maximizes profits and minimizes charity care. The 340B program is littered with problems, and it is crucial that Massachusetts takes steps to ensure that 340B is used properly and helps the patients it was intended to benefit.
About the Author
Matt Mulvey is a Roger Perry Transparency Intern at Pioneer Institute. He is a rising senior at Swarthmore College where he is a political science major and history minor.

